Introduction
Malocclusion is defined as an irregularity of the teeth or a molar relationship of the dental arches beyond the normal accepted range. It is a developmental problem determined mainly by hereditary and environmental factors. Any of these factors may influence the type and frequency of malocclusion in a given population. Most of the malocclusions can be corrected if detected early by correctional methods. Angle classified malocclusion as Class g0;,i5; and j4;,based on the relationship of the mesiobuccal cusp of the maxillary first molar and the buccal groove of the mandibular first molar.Class III malocclusion is considered to be one of the most difficult and complex orthodontic problems to treat. Prevalence of Class III malocclusion in North Indian population is stated to be 3.4% of the population in a study by Kharbanda et al in 1995.[1]
Class III malocclusion with an anterior crossbite is identified by the parents earlier than any other types of malocclusions. Many studies have reported that an early correction of anterior crossbite is of great significance for preventing the deterioration of the horizontal jaw relationship.[2] Timing of orthodontic treatment, especially for children with developing Class III malocclusions, has always been controversial.Therefore a definitive treatment plan tends to be delayed for severe Class III cases. The interaction between environmental and innate factors in the development of a Class III malocclusion has not been completely understood.Young Class III patients with moderate to severe anterior crossbite and deep bite do need early intervention in some selected cases.It is known that both anteroposterior and vertical maxillary deficiency can contribute to Class III malocclusion.If the maxilla does not grow vertically, the mandible rotates upward and forward, producing an appearance of a mandibular prognathism that may be attributed to both the position and the size of the mandible. In these cases, the mechanical interference by the overclosure of the mandible may influence the growth of maxilla and the alignment of the maxillary dentition. Also,many young children can benefit from treatment because it reduces the psychological burden of facial and dental disfigurements during some of their most formative years.[3]
This case report attempts to correct a developing Class j4; malocclusion at 2.5years of age.
Case Report
A 2.5 year old male child was brought to the Department of Paediatric and Preventive dentistry by his parents who complained of unesthetic appearence due to forward positioning of the child’s mandible. (Figure 1, 2)
 | Fig 1 : Pre Treatment Extraoral Photograph
 |
 | Fig 2 : Pre Treatment Extraoral Photograph
|
Clinical examination revealed an anterior crossbite in the deciduous dentition with a negative overjet of -1mm (Figure 3, 4) , a mild concave profile and a mesial step molar occlusion.
 | Fig 3 : Pre Treatment Intraoral Photograph
|
 | Fig 4 : Pre Treatment Intraoral Photograph
|
On examination,the parents of the patient exhibited a normal class 1 occlusion.
The patient exhibited the following positive factors-
a) A-P functional shift
b) Symmetrical condylar growth
c) Young with growth remaining
d) Mild skeletal disharmony
e) ANB<-2
f) No familial prognathism
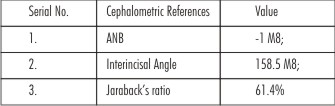 | The study of the pretreatment cephalogram(Figure 5) revealed the following values
|
The familial and medical history of the patient were not relevant.
Hence early treatment was initiated.
A cutomised acrylic chin cap was given with head support (Figure 6, 7) . This extraoral appliance has a head cap which is firmly seated on the posterosuperior aspects of the cranium as anchorage and has attachments for the placement and activation of a chin cup. A force module of elastic was used to provide desired tension levels on the chin cup itself (Figure 8, 9, 10).
 | Fig 6 : Chin Cap Made Of Acrylic
|
 | Fig 7 : Chin Cap Made Of Acrylic
|
 | Fig 8 : Etra-oral Photograph Of Patient With Chin Cap
|
 | Fig 9 : Etra-oral Photograph Of Patient With Chin Cap
|
 | Fig 10 : Etra-oral Photograph Of Patient With Chin Cap
|
The appliance was fabricated so that the pull on the chin cup was oriented along a line from the mandibular symphysis (pogonion) to the mandibular condyle.The patient was advised to wear the appliance continuously for 24 hours a day.
After 3 months of treatment an edge to edge bite was established,following which the chin cap appliance was tightened.(Figure 11, 12, 13, 14, 15, 16, 17)
 | Fig 11 : Intra-oral Mid-treatment Photograph
|
 | Fig 12 : Mid-treatment Extraoral Photograph
|
 | Fig 13 : Mid-treatment Extraoral Photograph
|
 | Fig 14 : Mid-treatment Extraoral Photograph
|
 | Fig 15 : Mid-treatment Extraoral Photograph With Chin Cap
|
 | Fig 16 : Mid-treatment Extraoral Photograph With Chin Cap
|
 | Fig 17 : Mid-treatment Extraoral Photograph With Chin Cap
|
The child started developing allergic rashes due to the acrylic chin cap which was changed to a customised chin cap made of cloth.(Figure 18, 19, 20, 21).
 | Fig 18 : Chin Cap Made Of Cloth
|
 | Fig 19 : Chin Cap Made Of Cloth
|
 | Fig 20 : Chin Cap Made Of Cloth
|
 | Fig 21 : Chin Cap Made Of Cloth
|
A positive overjet of 1mm was established after another 5 months (Figure 22, 23, 24).
 | Fig 22 : Post Treatment Intraoral Photograph
|
 | Fig 23 : Post Treatment Intraoral Photograph
|
 | Fig 24 : Post Treatment Intraoral Photograph
|
Result
After 5 months of treatment the following results were obtained –
The post treatment cephhalogram showed
1) An increase in the ANB angle from -1 M8; to +1 M8; -Indicating a correction of the crossbite (Figure25).
 | Fig 25 : Post Treatment Cephalogram
|
2) An increase in the Interincisal angle from 158.5 M8; to 166 M8; -Indicating the uprighting of the upper and lower incisors.
3) An increase in the Jaraback’s ratio from 61.4% to 64.8% -Indicating a shift from vertical growth pattern to horizontal growth pattern (Figure 26, 27, 28).
 | Fig 26 : Post Treatment Extraoral Photograph
|
 | Fig 27 : Post Treatment Extraoral Photograph
|
 | Fig 28 : Post Treatment Extraoral Photograph
|
4) The anterior crossbite was corrected to a positive overjet of +1mm.
Discussion
Many researchers have claimed the effectiveness of early treatment for Class j4; malocclusions. Nevertheless when analysing the studies in detail the initial age of Class j4; patients undergoing the 'early' treatment differs widely in the literature. A few authors have also reported the treatment of studies that were initiated as early as the deciduous dentition (Graber,1977;Ritucci and Nanda,1986;Stensland et al,1988)[4],[5],[6]. Sakamoto(1981)[7] noted a greater improvement of skeletal sagittal relationships in Japanese children with Class III malocclusions treated with chin cap from age of 3-5 years as compared to children treated at later ages. Mutschisch and Droll found that the very early treatment of Class III malocclusion offered the best chance for normal skeletal relationships[8]. Turpin(1981)[9] developed guidelines when to intercept Class III malocclusion. He suggested that if the patient showed characteristics in the positive column, early treatment should be considered. However if any characteristics fall in the negative column, delaying treatment until condylar growth has ceased may be the better alternative.
Chin cup therapy contributes to the correction of Class III malocclusion in several ways. First, by rotating the mandible posteriorly, the ramus is placed in a more vertical orientation to the upper craniofacial structures. Secondly, by overcoming the changes introduced by backward mandibular rotation, the gonial angle is decreased and the condylar growth is inhibited. Finally, vertical condylar growth is inhibited.[5],[10]
Conclusion
The aim of treating all developing Class j4;malocclusion is to enable the patient to close his jaws in normal centric relation without anterior interlock, thus permitting normal growth. This study demonstrated the achievement of significant results, and the stability of the corrected anterior crossbite associated with a developing Class III malocclusion treated with a chincup. Good results were achieved in this case. However,further long-term clinical investigations are necessary to assure the stability of Class III treatment.
References
1. Young-Min Moon; Sug-Joon Ahn; Young-Il Chang.Cephalometric Predictors of Long-term Stability in the Early Treatment of Class III Malocclusion.Angle Orthod 2005;75:747–753.
2. Zuisei Kannoa; Yoonji Kimb; Kunimichi Soma.Early Correction of a Developing Skeletal Class III Malocclusion.Angle Orthodontist 2007;77(3):549-56.
3. Baccetti T;Tollaro I.A retrospective comparison of functional appliance treatment of class 3 malocclusion in the deciduous and mixed dentition.European Journal of Orthodontics 1998;20:309-17.
4. Graber LW. Chincup therapy for mandibular prognathism.Am J Orthod. 1977;72:23–41.
5. RitucciR, Nanda R.The effect of chin cap on the growth and development of cranial base and midface.Am J Orthod.1986;90:475-86.
6. Stensland et al.Dentofacial changes in children with negative overjet treated by a combined orthopedic and orthodontic approach.European Journal of Orthodontics.1988;10:39-51.
7. Sakamoto T. Effective time for application of orthopedic force on skeletal class 3 malocclusion.Am J Orthod. 1981;80:411-16.
8. Philip M Campbell.The Dilemma of class 3 treatment:Early or late.Angle Orthodontist 1983;53(3):175-191.
9. Turpin;David L.Early class III treatment.Unpublished thesis presented at 81st session,Amer.Assoc. Orthodont.,San Francisco,1981.
10. Vego L. Early orthopedic treatment for Class III. Am J Orthod 1976;70:59-69. |